 2015, Vol. 42
2015, Vol. 42



调强放疗联合单药顺铂不同化疗方案同期治疗鼻咽癌的急性不良反应比较

本刊由国家卫生和计划生育委员会主管,湖北省卫生厅、中国抗癌协会、湖北省肿瘤医院主办。
文章信息
- 程金建,杨华,卢志平,陆合明,黄翌航,莫颖,陈甲信.2015.
- CHENG Jinjian, YANG Hua, LU Zhiping,LU Heming, HUANG Yihang, MO Ying,CHEN Jiaxin. 2015.
- 调强放疗联合单药顺铂不同化疗方案同期治疗鼻咽癌的急性不良反应比较
- Comparison of Acute Toxicity between Intensity-modulated Radiotherapy with Cisplatin Alone Concurrent Chemotherapy Weekly and Every Three Weeks for Nasopharyngeal Carcinoma Patients
- 肿瘤防治研究, 2015, 42(03): 285-289
- Cancer Research on Prevention and Treatment, 2015, 42(03): 285-289
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2015.03.016
-
文章历史
- 收稿日期:2014-03-21
- 修回日期:2014-10-10
引用本文 |
程金建,杨华,卢志平,陆合明,黄翌航,莫颖,陈甲信. 调强放疗联合单药顺铂不同化疗方案同期治疗鼻咽癌的急性不良反应比较[J]. 肿瘤防治研究, 2014, 03(42): 285-289.
CHENG Jinjian, YANG Hua, LU Zhiping,LU Heming, HUANG Yihang, MO Ying,CHEN Jiaxin. Comparison of Acute Toxicity between Intensity-modulated Radiotherapy with Cisplatin Alone Concurrent Chemotherapy Weekly and Every Three Weeks for Nasopharyngeal Carcinoma Patients. Cancer Research on Prevention and Treatment, 2014, 03(42): 285-289.
调强放疗联合单药顺铂不同化疗方案同期治疗鼻咽癌的急性不良反应比较
1. 530021 南宁,广西壮族自治区人民医院肿瘤中心放疗科;
2. 530021 南宁,广西医科大学药学院
2. 530021 南宁,广西医科大学药学院
摘要:目的 比较无远处转移鼻咽癌(nasopharyngeal carcinoma, NPC)调强放疗(intensity-modulatedradiotherapy,IMRT)联合单药顺铂每周(40 mg/m2,1次/周)和每3周(80~100 mg/m2,1次/3周)同期放化疗的急性不良反应和治疗前后的营养状况差异。方法回顾分析45例IMRT联合单药顺铂同期化疗的非转移NPC患者临床资料,急性不良反应评估采用CTCAE 3.0标准,不良反应和营养状况统计分析采用t检验、卡方分析或精确概率法以及方差分析检验。结果45例患者口干、咽痛、口腔黏膜炎、皮炎、恶心、呕吐及骨髓抑制3~4级不良反应发生率分别为6.7%、15.6%、28.9%、6.7%、8.9%、13.3%和22.2%。治疗后BW、BMI、TP、BUN、Cr、Na+、K+、Ca2+和Cl-变化的性别分层方差分析差异均无统计学意义(P>0.05),ALB变化接近统计学意义。组内分析显示两组治疗后ALB、TP、Na+和Cl-均下降(P<0.05),但顺铂每周组BW、BMI下降更明显(P<0.05)。结论治疗前后两组营养状况均有不同程度下降,顺铂每周组营养失衡较顺铂每3周组更普遍,但治疗前后两组变化无明显差异。
关键词:
鼻咽肿瘤
顺铂
放射疗法
高频
同期放化疗
急性不良反应
Comparison of Acute Toxicity between Intensity-modulated Radiotherapy with Cisplatin Alone Concurrent Chemotherapy Weekly and Every Three Weeks for Nasopharyngeal Carcinoma Patients
1. D Department of Radiation Oncology, Cancer Center, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning 530021, China;
2. School of Pharmaceutical Sciences, Guangxi Medical University, Nanning 530021, China
2. School of Pharmaceutical Sciences, Guangxi Medical University, Nanning 530021, China
Abstract:Objective To compare the acute toxicities and nutritional status between non-metastasis
nasopharyngeal carcinoma(NPC) patients treated by intensity-modulated radiotherapy(IMRT) combined with
40 mg/m² cisplatin alone concurrent chemotherapy weekly and those treated by IMRT with 80-100 mg/m2
cisplatin every three weeks. Methods A retrospective clinical data analysis was conducted on 45 patients
with non-metastatic NPC. Patients received 40 mg/m² cisplatin weekly or 80-100 mg/m2 cisplatin every three
weeks, concurrently with IMRT. The National Cancer Institute Common Toxicity Criteria version 3.0 scale
(CTCAE V3.0) was used to assess the chemotherapy and acute toxicities. The acute toxicities and nutritional
status were analyzed statistically by t-test, Chi-Square test/Chi-Square Goodness-of-Fit test or Analysis of
Variance (ANOVA).
Results In 45 NPC patients treated by IMRT, 31 patients received 40 mg/m² cisplatin
weekly and 14 patients received 80-100 mg/m2 cisplatin every three weeks concurrently chemotherapy. The
grade 3-4 acute toxicity occurrence rates of xerostomia, pharyngodynia, oral mucositis, dermatitis, nausea,
vomit and myelosuppression were 6.7%, 15.6%, 28.9%, 6.7%, 8.9%, 13.3% and 22.2%, respectively.
Although the changes of BW, BMI, ALB, TP, BUN, Cr, Na+, K+, Ca2+ and Cl- had no statistical difference
between two groups after treatment(P>0.05) by Gender stratification ANOVA, the change of ALB was closed
to a statistical difference. Both groups of ALB, TP, Na+ and Cl- were decreased after treatment (P<0.05),
but BW and BMI in cisplatin weekly group were decreased more severely than those in cisplatin every three
weeks group.
Conclusion In 45 NPC patients treated by IMRT, 31 patients received 40 mg/m² cisplatin
weekly and 14 patients received 80-100 mg/m2 cisplatin every three weeks concurrently chemotherapy. The
grade 3-4 acute toxicity occurrence rates of xerostomia, pharyngodynia, oral mucositis, dermatitis, nausea,
vomit and myelosuppression were 6.7%, 15.6%, 28.9%, 6.7%, 8.9%, 13.3% and 22.2%, respectively.
Although the changes of BW, BMI, ALB, TP, BUN, Cr, Na+, K+, Ca2+ and Cl- had no statistical difference
between two groups after treatment(P>0.05) by Gender stratification ANOVA, the change of ALB was closed
to a statistical difference. Both groups of ALB, TP, Na+ and Cl- were decreased after treatment (P<0.05),
but BW and BMI in cisplatin weekly group were decreased more severely than those in cisplatin every three
weeks group.
Key words:
Nasopharyngeal neoplasms
Cisplatin
Radiotherapy
Intensity-modulated
Concurrent chemoradiotherapy
Acute adverse reaction
0 引言
2.3 IMRT联合单药顺铂每周和每3周同期化疗
NPC患者的营养状况比较
3 讨论
目前顺铂为主的同期放化疗是局部晚期鼻咽癌 (nasopharyngeal carcinoma,NPC)的主要根治方 案,调强放疗(intensity-modulated radiotherappy, IMRT)既能提高肿瘤靶区适形度、保护风险器 官,还能减轻急性、晚期不良反应发生率和改善 生活质量[1,2],甚至能提高肿瘤局部控制率和总生 存率[3,4],因此,IMRT联合单药顺铂同期化疗逐渐 成为NPC主流治疗模式。最新版美国NCCN指南和 2010年NCCN指南(中国版)头颈部肿瘤临床实践 指南推荐放疗联合单药顺铂同期化疗作为NPC首选 治疗方案[5],单药顺铂同期化疗方案有两种推荐, 100 mg/m2,1次/3周和40 mg/m2,1次/周。本研究 回顾分析IMRT联合指南推荐的单药顺铂方案同期 化疗NPC患者的临床资料,比较单药顺铂每周方案 (40 mg/m2,1次/周)和每3周方案(100 mg/m2,1 次/3周)的急性不良反应和治疗前后患者的营养状 况变化,探索两种同期放化疗方案对NPC患者的不 同影响,为临床治疗提供依据。 1 资料与方法 1.1 研究对象
广西壮族自治区人民医院肿瘤中心放疗科 2007年11月至2010年11月收治的无远处转移、 IMRT联合单药顺铂同期化疗的NPC患者为研究对 象,收集整理相关临床资料,符合研究标准并具 有完整研究资料的患者共45例。 1.2 调强放疗方式
采用头后伸仰卧位,头颈肩面罩固定,增强 CT扫描(颅顶至锁骨头下2 cm,2~3 mm /层), 计划系统采用Nucletron或CMS。影像资料可见肿 瘤为原发灶(GTVnx)和淋巴结区(GTVnd), GTVnx、GTVnd外扩3~5 mm为临床肿瘤体积 (CTVnx/nd);临床肿瘤体积1(CTV1)包括颅 底、上颌窦后部、鼻腔后1/3、后组筛窦、蝶窦下 部、咽旁间隙、咽后间隙、翼突、翼腭窝以及阳性 淋巴结的颈部分区;临床肿瘤体积2(CTV2)为阳 性淋巴结区域以外的颈部和锁骨阴性淋巴结区。 计划肿瘤体积(PTVs)为CTVs外扩2~5 mm,规 避脑干、脊髓、晶体等器官,处方剂量为:PTVnx 68~78 Gy,PTVnd 68~76 Gy包括鼻咽部和(或) 转移淋巴结残留加量,PTV1 55.8~68 Gy,PTV2 50.4~60 Gy,分割剂量1.8~2.3 Gy/d,5次/周。 1.3 同期化疗方案
45例NPC患者均为单药顺铂同期化疗,31例 患者采用40 mg/m2,1次/周,平均化疗(5.2±1.4) 周期,其中1例3周期同期化疗后因严重不良反应 改为奈达铂单药,同期化疗6周期;另外14例患 者采用80~100 mg/m2,1次/3周,平均化疗(2.2± 0.6)周期。同期化疗于IMRT第1或第2天开始。 1.4 研究方法
收集45例NPC患者IMRT前后体重、身高、营 养元素和不良反应等临床资料,由公式计算身体 质量指数(BMI)=体重/身高2 。比较分析放疗前 后患者体重、BMI及营养状况变化和不良反应。 放化疗急性不良反应评估采用CTCAE 3.0标准。 1.5 统计学方法
采用IBM SPSS20.0统计软件包,实验数据正态分 布以(x±s)表示,数据比较用两独立样本t检验和方 差分析,非正态分布数据分析采用卡方检验或Fisher 精确检验,P<0.05为差异有统计学意义。 2 结果 2.1 IMRT联合单药顺铂每周和每3周同期化疗方 案一般情况比较
两组患者除性别外,年龄、病理分级、PS评 分、T、N、M分期和临床分期组间差异均无统计 学意义,见表 1。
表 1 45例鼻咽癌患者的一般临床特点和治疗方案 (n=45)
Table 1 General clinical characteristics and treatment of
NPC patients (n=45)
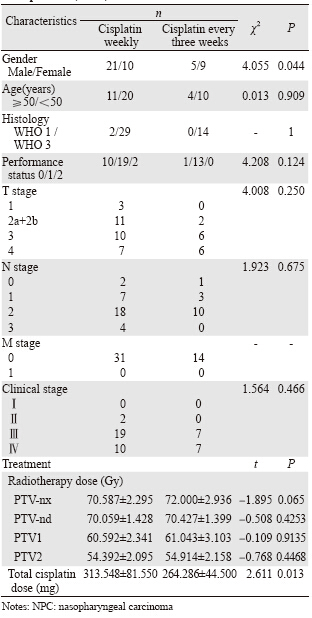 |
治疗方案显示两组患者顺铂总剂量存在组间 差异,而放疗靶区PTVnx、PTVnd、PTV1、PTV2 放疗剂量均无组间差异。 2.2 IMRT联合单药顺铂每周和每3周同期化疗的 不良反应比较
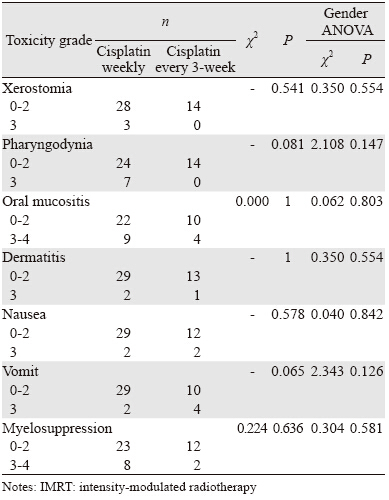
本研究45例NPC患者口干、咽痛、口腔黏膜 炎、皮炎、恶心、呕吐及骨髓抑制3~4级不良反 应发生率分别为6.7%、15.6%、28.9%、6.7%、 8.9%、13.3%和22.2%。31例单药顺铂每周和14例 每3周同期放化疗患者0~2级和3~4级口干、咽痛、 口腔黏膜炎、皮炎、恶心、呕吐及骨髓抑制等不 良反应差异均无统计学意义(P>0.05),其中咽 痛及呕吐反应接近统计学意义。性别分层方差分 析提示两组患者放化疗不良反应差异均无统计学 意义(P>0.05),见表 2。
表 2 鼻咽癌调强放疗联合单药顺铂每周和每3周方案同期
化疗的不良反应比较(n=45)
Table 2 Toxicity of IMRT combined with cisplatin alone
concurrent chemotherapy weekly and every three weeks for
NPC patients(n=45)
 |
除了顺铂每周方案的血清肌酐外,两组方案 治疗后营养元素值均较治疗前有不同程度下降。 统计分析显示IMRT联合两种单药顺铂同期化疗 方案治疗前患者BW、BMI、ALB、TP、BUN、 Cr、Na+、K+、Ca+和Cl-差异无统计学意义(P> 0.05)。组内比较显示,两组治疗后ALB、TP、 Na+和Cl-较治疗前下降(P<0.05),顺铂每周组 BW、BMI下降更明显(P>0.05)。性别分层方差 分析显示,治疗前后两组BW、BMI、TP、BUN、 Cr、Na+、K+、Ca+和Cl-变化差异均无统计学意义 (P>0.05),ALB变化差异接近统计学意义,见 表 3。另外,顺铂每周方案组有1例出现一过性急 性肾功能不全,3周方案组无肾功能异常出现。
表 3 IMRT联合单药顺铂每周和每3周同期放化疗NPC患者的营养状况比较(n=45)
Table 3 Nutritional status of IMRT combined with cisplatin alone concurrent chemotherapy weekly and every three weeks
for NPC patients(n=45)
 |
目前研究显示局部晚期NPC辅助化疗并未带 来生存获益,尽管诱导化疗联合同期放化疗被 NCCN指南推荐,但其作用和地位尚未被完全肯 定[6,7]。单药顺铂同期放化疗仍是NPC的标准治疗 方案。文献报道IMRT联合单药顺铂同期放化疗 使NPC患者5年总生存率提高至80%左右,早期 患者5年生存率高于95%,部分报道达100%[8,9]。 研究显示顺铂同期化疗的总剂量与NPC患者的总 生存率和无复发生存率有关[10]。还有研究发现 Ⅱ、Ⅲ期同期放化疗的NPC患者,顺铂每周同期 化疗5周期以上、总剂量>200 mg/m2者的总生存 明显高于5周期以下、顺铂总剂量<200 mg/m2 的患者[11],提示顺铂同期化疗的总剂量与疗效相 关。Chen的研究显示,与单纯放疗比较,顺铂同 期放化疗可以提高Ⅱ期NPC的5年总生存率、无 病生存率以及无远处转移生存率,但没有提高局 部和区域控制率,而白细胞减少、口腔黏膜炎、 恶心和呕吐等急性不良反应明显增加,晚期不良 反应增加不明显[12]。还有研究也显示单药顺铂同 期放化疗能提高局部晚期NPC患者的总生存率, 但不良反应发生率也明显增加,尤以3~4级血液 学毒性和口黏膜炎最为常见[6,13,14,15]。Liu发现,与 单纯放疗比较,同期放化疗能提高成人合并症评 测-27(ACE-27)评分小于2分的老年NPC患者5 年总生存率、肿瘤特异性生存率和无病生存率, 但无转移生存率无明显提高,而对2分以上老年 患者5年总生存率无明显改善[16]。极少数研究显 示顺铂同期放化疗对NPC总生存改善不明显,反而 增加了严重不良反应[9],甚至提高了死亡风险[17]。 本研究组前期研究IMRT联合顺铂每周同期化疗 显示95.5%患者可完成既定方案治疗,22例患者 3~4级口腔黏膜炎发生率达27%,其余3~4级急性 不良反应发生率小于10%[18]。由此可见,多数研 究认为鼻咽癌顺铂同期放化疗的疗效值得肯定, 但同期放化疗的急性不良反应发生率高于单纯放 疗,值得重视。另外,顺铂同期化疗的总剂量可 能与NPC预后有关。高效、低毒、合理的NPC同 期放化疗方案仍待探索。
本研究比较无远处转移NPC患者IMRT联合 两种单药顺铂同期化疗的急性不良反应和营养状 况,结果显示45例患者口腔黏膜炎和骨髓抑制3~4 级不良反应超过20%,其余均小于20%,与文献报 道类似。单药顺铂每周和每3周同期化疗的口干、 咽痛、口腔黏膜炎、皮炎、恶心、呕吐及骨髓抑制 0~2级和3~4级不良反应差异无统计学意义,提示 两种方案联合IMRT的急性不良反应基本类似。营 养状况比较结果显示,治疗后BW、BMI、ALB、 TP、BUN、Na+、K+、Ca+和Cl-均有不同程度下 降,但两组同期放化疗方案无组间差异。组内分 析结果提示顺铂每周同期化疗组BW、BMI减轻以 及营养不良状况似乎较3周组更明显,可能与每周 同期化疗时顺铂的总剂量较高有关,还有可能因 为每周同期化疗时顺铂累积毒性和持续作用,导 致患者恶心、呕吐以及食欲不振,治疗期间营养 摄入减少有关。不少研究显示NPC患者放化疗期 间会出现不同程度的营养不良及体重减轻[19,20,21,22]。还 有研究报道鼻咽癌IMRT患者营养状况改变可能影 响IMRT计划[23,24]。可见,IMRT联合顺铂同期放化 疗NPC患者的营养状况变化值得重视。
总之,顺铂同期放化疗提高了NPC患者的总 生存率,但同期放化疗的急性不良反应较单纯放 疗明显增加。鼻咽癌IMRT联合单药顺铂每周和每 3周同期放化疗的急性不良反应差别可能不明显, 但治疗前后均有不同程度营养失衡,似乎单药顺 铂每周同期化疗方案营养状况改变较3周方案更普 遍,而两种方案疗效差异有待比较。由于样本量 和回顾性研究方法等因素限制,鼻咽癌高效、低 毒、安全、合理的单药顺铂同期放化疗方案有待 多中心、大样本、前瞻性临床研究证实。
参考文献
| [1] | Liu XQ, Luo W, Tang YQ, et al. A matched cohort analysis ofthree-dimensional conformal radiotherapy versus conventionalradiotherapy for primary nasopharyngeal carcinoma[J]. Ai Zheng,2008, 27(6): 606-11.[刘晓清, 罗伟, 汤轶强, 等. 三维适形与常规二维放射治疗初治鼻咽癌的配对设计队列研究[J]. 癌症, 2008,27(6): 606-11.] |
| [2] | Fang FM, Chien CY, Tsai WL, et al. Quality of life and survivaloutcome for patients with nasopharyngeal carcinoma receivingthree-dimensional conformal radiotherapy vs. intensity-modulatedradiotherapy-a longitudinal study[J]. Int J Radiat Oncol Biol Phys,2008, 72(2): 356-64. |
| [3] | Fang FM, Tsai WL, Chen HC, et al. Intensity-modulated orconformal radiotherapy improves the quality of life of patientswith nasopharyngeal carcinoma: comparisons of four radiotherapytechniques[J]. Cancer, 2007, 109(2): 313-21. |
| [4] | Lai SZ, Li WF, Chen L, et al. How does intensity-modulatedradiotherapy versus conventional two-dimensional radiotherapyinfluence the treatment results in nasopharyngeal carcinomapatients?[J]. Int J Radiat Oncol Biol Phys, 2011, 80(3): 661-8. |
| [5] | National Comprehensive Cancer Network. NCCN Clinical PracticeGuidelines in Oncology: head and neck cancers,V.2.2013[s]. http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.Accessed March 8, 2014. |
| [6] | Chen L, Hu CS, Chen XZ, et al. Concurrent chemoradiotherapyplus adjuvant chemotherapy versus concurrent chemoradiotherapyalone in patients with locoregionally advanced nasopharyngealcarcinoma: a phase 3 multicentre randomised controlled trial[J].Lancet Oncol, 2012, 13(2): 163-71. |
| [7] | Fountzilas G, Ciuleanu E, Bobos M, et al. Induction chemotherapyfollowed by concomitant radiotherapy and weekly cisplatinversus the same concomitant chemoradiotherapy in patientswith nasopharyngeal carcinoma: a randomized phase Ⅱ studyconducted by the Hellenic Cooperative Oncology Group (HeCOG)with biomarker evaluation[J]. Ann Oncol, 2012, 23(2): 427-35. |
| [8] | Xu L, Pan J, Wu J, Pan C, et al. Factors associated with overallsurvival in 1706 patients with nasopharyngeal carcinoma:significance of intensive neoadjuvant chemotherapy and radiationbreak[J]. Radiother Oncol, 2010, 96(1): 94-9. |
| [9] | Sun X, Su S, Chen C, et al. Long-term outcomes of intensitymodulatedradiotherapy for 868 patients with nasopharyngealcarcinoma: an analysis of survival and treatment toxicities[J].Radiother Oncol, 2014, 110(3): 398-403. |
| [10] | Lee AW, Tung SY, Ngan RK, et al. Factors contributing to theefficacy of concurrent–adjuvant chemotherapy for locoregionallyadvanced nasopharyngeal carcinoma: combined analyses ofNPC-9901 and NPC-9902 trials[J]. Eur J Cancer, 2011, 47(5):656-66. |
| [11] | Loong HH, Ma BB, Leung SF, et al. Prognostic significanceof the total dose of cisplatin administered during concurrentchemoradiotherapy in patients with locoregionally advancednasopharyngeal carcinoma[J]. Radiother Oncol, 2012, 104(3):300-4. |
| [12] | Chen QY, Wen YF, Guo L, et al. Concurrent chemoradiotherapyvs. radiotherapy alone in stage Ⅱ nasopharyngeal carcinoma:phase Ⅲ randomized trial[J]. J Natl Cancer Inst, 2011, 103(23):1761-70. |
| [13] | Lee AW, Tung SY, Chan AT, et al. Preliminary results of arandomized study (NPC-9902 Trial) on therapeutic gain byconcurrent chemotherapy and/or accelerated fractionation forlocally advanced nasopharyngeal carcinoma[J]. Int J Radiat OncolBiol Phys, 2006, 66(1): 142-51. |
| [14] | Chen Y, Liu MZ, Liang SB, et al. Preliminary results ofa prospective randomized trial comparing concurrentchemoradiotherapy plus adjuvant chemotherapy with radiotherapyalone in patients with locoregionally advanced nasopharyngealcarcinoma in endemic regions of China[J]. Int J Radiat Oncol BiolPhys, 2008, 71(5): 1356-64. |
| [15] | Ohno T, Thinh DH, Kato S, et al. Radiotherapy concurrentlywith weekly cisplatin, followed by adjuvant chemotherapy, forN2–3 nasopharyngeal cancer: a multicenter trial of the Forumfor Nuclear Cooperation in Asia[J]. J Radiat Res, 2013, 54(3):467-73. |
| [16] | Liu H, Chen QY, Guo L, et al. Feasibility and efficacy ofchemoradiotherapy for elderly patients with locoregionallyadvanced nasopharyngeal carcinoma: results from a matchedcohort analysis[J]. Radiat Oncol, 2013, 8: 70. |
| [17] | Zhang AM, Fan Y, Wang XX, et al. Increased treatment-relatedmortality with additional cisplatin-based chemotherapy in patientswith nasopharyngeal carcinoma treated with standard radiotherapy[J]. Radiother Oncol, 2012, 104(3): 279-85. |
| [18] | Lu H, Chen J, Huang B, et al. Feasibility and efficacy study ofweekly cisplatin with concurrent intensity-modulated radiationtherapy for nasopharyngeal carcinoma: preliminary results[J].Oral Oncol, 2010, 46(10): 743-7. |
| [19] | Ng K, Leung SF, Johnson PJ, et al. Nutritional consequences ofradiotherapy in nasopharynx cancer patients[J]. Nutr Cancer,2004, 49(2): 156-61. |
| [20] | Oates JE, Clark JR, Read J, et al. Prospective evaluation of qualityof life and nutrition before and after treatment for nasopharyngealcarcinoma[J]. Arch Otolaryngol Head Neck Surg, 2007, 133(6):533-40. |
| [21] | Cheng JJ, Yang H, Chen JX, et al. The impacts of intensitymodulatedradiotherapy and chemotherapy on nutritional status ofpatients with nasopharyngeal carcinoma[J]. Guangdong Yi Xue,2011, 32(17): 2336-8.[程金建, 杨华, 陈甲信, 等. 调强放疗及化疗对鼻咽癌患者营养状况的影响[J] . 广东医学, 2011, 32(17):2336-8.] |
| [22] | Cheng JJ, Yang H, Lu HM, et al. Analysis of body weight lossand influence factors during intensity-modulated radiotherapy forpatients with nasopharyngeal carcinoma[J]. Zhong Liu Fang ZhiYan Jiu, 2013, 40(8): 767-71.[程金建, 杨华, 陆合明, 等. 鼻咽癌患者调强放疗过程中体重变化及影响因素分析[J]. 肿瘤防治研究, 2013, 40(8): 767-71.] |
| [23] | Wang X, Lu J, Xiong X, et al. Anatomic and dosimetric changesduring the treatment course of intensity-modulated radiotherapyfor locally advanced nasopharyngeal carcinoma[J]. Med Dosim,2010, 35(2): 151-7. |
| [24] | Wang W, Yang H, Hu W, et al. Clinical study of the necessity ofreplanning before the 25th fraction during the course of intensitymodulatedradiotherapy for patients with nasopharyngealcarcinoma[J]. Int J Radiat Oncol Biol Phys, 2010, 77(2): 617-21. |