
Significance of Content and Integrity Changes of Peripheral Blood Cell-free DNA in Diagnosis and Treatment in Gastric Cancer
-
摘要:目的
监测胃癌患者外周血游离DNA(cell-free DNA, cf-DNA)的含量,探讨其在胃癌诊治和预后中的价值。
方法收集81例原发胃癌、18例胃良性肿瘤、19例胃癌前病变、43例同期门诊健康体检者以及部分术后和随访的外周血标本,提取游离DNA,荧光定量PCR检测其含量(ALU115和ALU247)并计算完整性(ALU247/ALU115),分析血清游离DNA和血浆游离DNA含量之间的相关性。
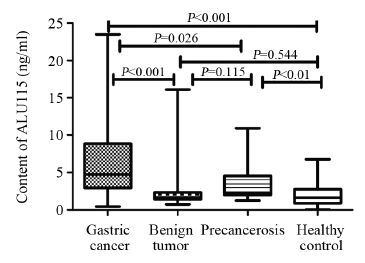
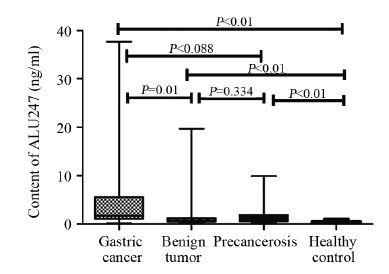
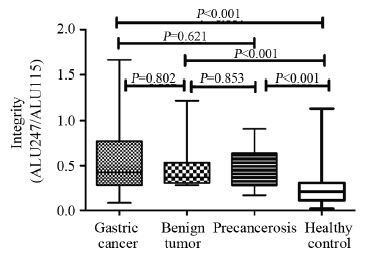
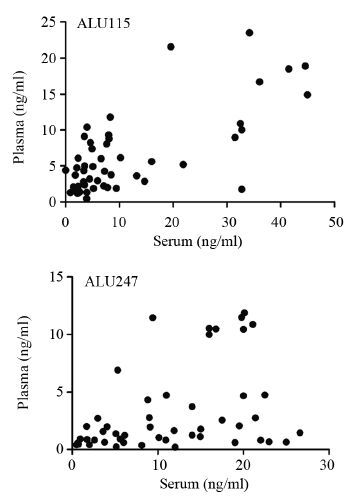
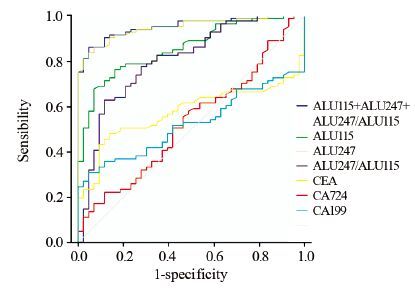
结果血浆游离DNA含量和完整性在四组之间的差异有统计学意义(ALU115、ALU247以及完整性的P值均<0.001),术前术后的差 异也有统计学意义(P值分别为0.000、0.013、0.010),随访前后完整性差异有统计学意义(P=0.029),在有无转移、分期、分化程度间差异有统计学意义(P值分别为0.013、0.042、0.003)。血浆和血清游离DNA含量具有相关性且血浆离散趋势更小。ALU247的ROC曲线下面积最高(0.985)。
结论游离DNA检测在胃癌的诊治和预后中有一定的价值。
Abstract:ObjectiveTo explored the role and value in the diagnosis, treatment and prognosis in gastric cancer via monitoring the content of cell-free DNA(cf-DNA).
Methodswe collected preoperative peripheral blood specimens from 81 cases of patients with primary gastric cancer, 18 cases gastric benign tumors, 19 cases gastric precancerous lesion, 43 cases of corresponding healthy controls. We also collected part of the postoperative and follow-up specimens. cf-DNA from specimens was extracted and used to detect the content and integrity of two DNA genes (ALU115 and ALU247) by fluorescence quantitative PCR. We compare the correlation of cf-DNA in serum and plasma.
ResultsThe content and integrity of cf-DNA have statistically significant difference in four groups, in pre- and post- operation and follow-up specimens,in staging, differentiated degree and with or without metastasis (P<0.05). The content of cf-DNA in plasma and serum is relevant and the former has less discrete trend. The area under the curve (AUC) of ALU247 was 0.985.
ConclusionThe test of cf-DNA has certain value in the diagnosis, treatment and prognosis of gastric cancer.
-
Key words:
- cell-free DNA /
- DNA Integrity /
- Tumor markers
-
0 引言
白血病发病率相对较小[1],但生存率较低(19.6%)[2],因此,严重影响儿童及老年人的身体健康,是造成居民巨大疾病负担的癌症之一[3-4]。昆山市位居上海与苏州之间,特殊的区位优势使得近20年经济社会快速发展,在昆山市肿瘤粗死亡率明显上升的背景下[5],本研究利用1993—2014年昆山市死因监测的白血病死亡数据,以探究其死亡率的时间趋势。
1 资料与方法
1.1 研究对象来源
江苏省昆山市于1981年全面开展全人群死因监测工作[5]。昆山市所有社区卫生服务机构及医院开展死因常规监测,同时疾控中心通过定期与公安、殡葬、妇幼保健及福利院等多部门合作,多途径收集死亡名单并开展死亡原因调查;市镇两级从业人员通过定期举办培训班、认真规范填写死亡证、逐条数据审核、现场督导检查及定期开展漏报调查等方式,来保证全市死因监测工作的质量。此外,也与苏州市范围内的其他县(市)进行数轮的数据质量互审,重点对数据的完整性、原始数据的逻辑性、统计分类及ICD-10编码以及是否重卡等进行检查、修正。昆山市所有死亡病例开具《居民死亡医学证明(推断)书》其登记报告项目包括:(1)病例人口学特征(姓名、性别、出生日期、民族、婚姻、文化程度、职业等)。(2)死亡信息:死亡原因(直接死因、间接死因、根本死因以及其他重要医学情况)、死亡日期、死亡地点等。(3)诊断信息:疾病最高诊断单位、疾病最高诊断依据等内容。(4)调查记录。年初与年末人口数来源于昆山市公安局,以计算年均观察人年数,1981—2013年年均观察人年数(年均人口数)详参文献[5]。
按照《国际疾病分类》(ICD-10)对所有恶性肿瘤疾病进行编码,白血病ICD-10编码为C91-95。根据《中国肿瘤登记工作指导手册》,并参照国际癌症研究中心(IARC)/国际癌症登记协会(IACR)对登记材料的有关要求,对肿瘤登记的完整性和可靠性进行了评估。
1.2 数据分析
采用SAS9.3统计软件进行数据分析,计算年份、性别粗死亡率与年龄标化死亡率,以及绘制时间趋势图和年龄别死亡率序列图。按照第五次全国人口普查(2000年)人口结构为标准计算年龄标化死亡率。应用年度变化百分比(annual percentage change, APC)及其95%可信区间(confidence intervals, CI)分析粗死亡率与年龄标化死亡率等时间趋势,以APC其95%CI是否包含0为统计学检验标准,同时给出回归系数检验的P值[6]。
2 结果
2.1 江苏省昆山市1993—2014年白血病死亡趋势分析
江苏省昆山市1993—2014年期间白血病死亡总例数为570例(男312例,女258例),占全肿瘤比例为2.19%;总的来看昆山市1993—2014年白血病死亡数明显上升(APC=3.0, 95%CI: 1.6~4.4, P=0.0007)。
江苏省昆山市白血病粗死亡率由1993年的4.01/10万上升到2014年的4.99/10万,上升趋势没有统计学意义(APC=1.5, 95%CI: 0.0~3.0, P=0.0604)。在男性人群中白血病粗死亡率由1993年的4.53/10万上升到2014年的5.02/10万,上升趋势无明显统计学意义(APC=0.8, 95%CI: -0.6~2.2, P=0.2756);女性人群中白血病粗死亡率由1993年的3.49/10万上升到2014年的4.96/10万,上升趋势无统计学意义(APC=2.7, 95%CI: 0.0~5.4, P=0.0622)。1993—2014年白血病中标死亡率在男女合计人群中无明显变化趋势(APC=1.5, 95%CI: 0.0~3.0, P=0.0604);男性(APC=-0.7, 95%CI: -2.4~1.0, P=0.4087)和女性(APC=0.4, 95%CI: -2.3~3.1, P=0.7612)人群中白血病中标死亡率没有明显变化趋势,见图 1、表 1。
1993—2014年白血病死亡率其0~74岁累积死亡率由1993年的0.33%上升到2014年的0.38%(APC=0.7, 95%CI: -0.9~2.3, P=0.4168),没有发现白血病死亡的风险在0~74岁年龄组随着时间有明显变化,见表 1。
![]() 图 1 江苏省昆山市1993—2014年白血病死亡率趋势图Figure 1 Age standardized rate of mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2014表 1 江苏省昆山市1993—2014年白血病死亡率分析Table 1 Mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2014
图 1 江苏省昆山市1993—2014年白血病死亡率趋势图Figure 1 Age standardized rate of mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2014表 1 江苏省昆山市1993—2014年白血病死亡率分析Table 1 Mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2014
2.2 江苏省昆山市1993—2014年白血病年龄别死亡率分析
1993—2004年,白血病年龄别死亡率在60之前处于低水平,60岁以后缓慢上升,至65~69岁达到高峰,70岁以后白血病死亡率明显下降。2005—2014年,白血病年龄别死亡率在60之前处于低水平,60岁以后开始明显抬升,至70~74岁达到高峰,75岁以后白血病死亡率略有下降。与1993—2004年相比,2005—2014年白血病年龄别死亡率明显偏高,特别是60岁以上年龄段,见图 2、表 2。
![]() 图 2 江苏省昆山市白血病年龄别死亡率在两个时期的比较Figure 2 Age-specific mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2004 and 2005-2014表 2 江苏省昆山市白血病年龄别死亡率分析Table 2 Age-specific mortality of leukemia by gender in Kunshan City, Jiangsu Province
图 2 江苏省昆山市白血病年龄别死亡率在两个时期的比较Figure 2 Age-specific mortality of leukemia in Kunshan City, Jiangsu Province, 1993-2004 and 2005-2014表 2 江苏省昆山市白血病年龄别死亡率分析Table 2 Age-specific mortality of leukemia by gender in Kunshan City, Jiangsu Province
3 讨论
在江苏省昆山市肿瘤中标死亡率总体呈现下降趋势的情况下[5],人口老龄化与其他危险因素一起促进了肿瘤死亡的变化。在昆山市肿瘤死亡率明显上升的肺癌中这种促进因素最为明显[7]。虽然昆山市白血病占全肿瘤死亡(2.19%)的比例较低;但是由于发病年龄较早、生存率较低及预后差[2],造成的疾病负担较大。
昆山市白血病死亡率位居肿瘤死亡顺位第9位[8-9]。同期与全国白血病死亡率相比,昆山地区死亡率明显低于全国2009年水平(世标率,2.66/10万 vs. 3.35/10万)[10],也低于全国2012年水平(2.48/10万 vs. 3.13/10万)[11]。就死亡率趋势来看,昆山市1993—2014年白血病中标死亡率趋势则没有明显的变化(APC=1.5, 95%CI: 0.0~3.0, P=0.0604)。浙江省2000—2009年白血病死亡率明显上升(APC=5.09, 95%CI: 1.13~9.21)[12],此外还有山东省(1970—2005年)[13]。除了单独看白血病死亡率,白血病发病率的高低不容忽视。与昆山市相邻的浙江省2000—2009年白血病的发病率明显上升(APC=3.21, 95%CI: 0.20~6.30)[12],此外上海[14]与南京地区[4]白血病发病率也明显上升。
从白血病年龄别死亡率来看,本研究显示白血病年龄别死亡率呈现明显的两个高峰,即20岁以下年龄组与65岁以上年龄组,与上海和浙江等地区的研究结果基本一致[4, 12, 14];也与全国肿瘤登记的结果一致[15]。年龄别死亡率的差异提示白血病的发病可能是暴露因素的差异所致。白血病的发生是基因与环境共同作用的结果。经济社会状态也是影响白血病发生的因素[16]。环境因素中饮食模式是影响白血病发生的因素之一[17-18];父母早期的不良生活方式暴露是影响儿童白血病的因素,如烟草、酒精等[19-20]。
虽然江苏省昆山市1993—2014年白血病死亡率趋势变化不明显;但是随着户籍人口逐年增加,因白血病而死亡的例数明显上升,疾病负担加大。在继续强化监测工作以观察其时间趋势的同时,也要考虑进一步加强监测工作质量控制。江苏省昆山市于1981年全面开展死因监测[5];在2013年加入国家疾病监测点,在加入监测点之前于2011—2012年开展了死亡漏报调查,结果显示漏报率为0.34%,提示既往的死因监测处于可接受区间[21]。
-
![]()
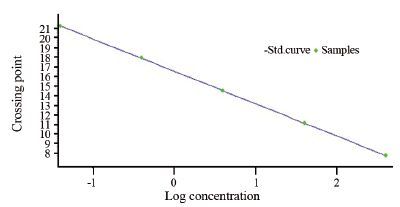
图 1 内参基因β-actin扩增的标准曲线
Figure 1 The standard curve of reference gene beta-actin amplification
![]()
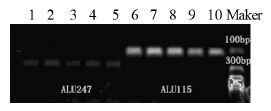
图 2 ALU115和ALU247两片段电泳图
Figure 2 Electrophoresis of the two segments (ALU115 and ALU247)
![]()
图 6 ALU115片段、ALU247片段血清和血浆相关性比较散点图
Figure 6 ALU115 fragment,ALU247 fragment serum and plasma correlation comparison scatter plot
![]()
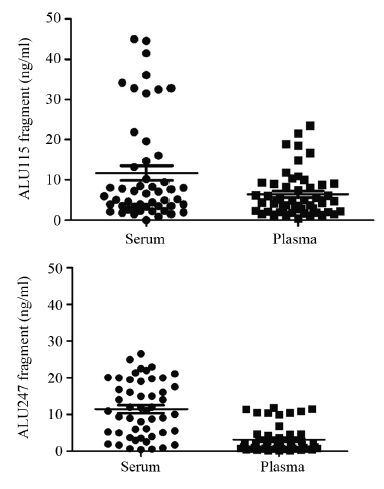
图 7 ALU115片段、ALU247片段血清和血浆游离DNA含量散点图
Figure 7 Scatter plots of ALU115 fragment,ALU247 fragment serum and plasma cf-DNA content
表 2 各组之间ALU115、ALU247以及ALU247/ALU115的值(中位数(四分位数))
Table 2 Values of ALU115,ALU247,and ALU247/ALU115 in each group (Median (Quartiles))

 下载: 导出CSV
下载: 导出CSV
表 3 胃癌患者临床病理参数与血浆游离DNA的相关性
Table 3 Correlation between clinical pathological parameters and plasma free DNA in patients with gastric cancer
 下载: 导出CSV
下载: 导出CSV
表 4 术前、术后和随访血浆游离DNA含量和完整性数据表 (中位数(四分位数))
Table 4 Preoperative,postoperative and follow up plasma free DNA content and integrity data sheet (Median (Quartiles))
 下载: 导出CSV
下载: 导出CSV
-
[1] Umetani N, Giuliano AE, Hiramatsu SH, et al. Prediction of breast tumor progression by integrity of free circulating DNA in serum[J]. J Clin Oncol, 2006, 24(26): 4270-6. doi: 10.1200/JCO.2006.05.9493
[2] CHUN FKH, Mueller I, Lange I, et al. Circulating tumour-associated plasma DNA represents an independent and informative predictor of prostate cancer[J]. BJU Int, 2006, 98(3): 544-8. doi: 10.1111/bju.2006.98.issue-3
[3] Tomita H, Ichikawa D, Ikoma D, et al. Quantification of circulating plasma DNA fragments as tumor markers in patients with esophageal cancer[J]. Anticancer Res, 2007, 27(4C): 2737-41.
[4] Gang F, Guorong L, An Z, et al. Prediction of clear cell renal cell carcinoma by integrity of cell-free DNA in serum[J]. Urology, 2010, 75(2): 262-5. doi: 10.1016/j.urology.2009.06.048
[5] Park JL, Kim HJ, Choi BY, et al. Quantitative analysis of cell-free DNA in the plasma of gastric cancer patients[J]. Oncology Lett, 2012, 3(4): 921-6.
[6] Choi JJ, Reich CF 3rd, Pisetsky DS. The role of macrophages in the in vitro generation of extracellular DNA from apoptotic and necrotic cells[J]. Immunology, 2005, 115(1): 55-62. doi: 10.1111/imm.2005.115.issue-1
[7] Jahr S, Hentze H, Englisch S, et al. DNA fragments in the blood plasma of cancer patients: quantitations and evidence for their origin from apoptotic and necrotic cells[J]. Cancer Res, 2001, 61(4): 1659-65.
[8] Mouliere F, El Messaoudi S, Pang D, et al. Multi-marker analysis of circulating cell-free DNA toward personalized medicine for colorectal cancer[J]. Mol Oncol, 2014, 8(5): 927-41. doi: 10.1016/j.molonc.2014.02.005
[9] Kim K, Shin DG, Park MK, et al. Circulating cell-free DNA as a promising biomarker in patients with gastric cancer: diagnostic validity and significant reduction of cfDNA after surgical resection[J]. Ann Surg Treat Res, 2014, 86(3): 136-42. doi: 10.4174/astr.2014.86.3.136
[10] Lee YJ, Yoon KA, Han JY, et al. Circulating cell-free DNA in plasma of never smokers with advanced lung adenocarcinoma receiving gefitinib or standard chemotherapy as first-line therapy[J]. Clin Cancer Res, 2011, 17(15): 5179-87. doi: 10.1158/1078-0432.CCR-11-0400
[11] Agostini M, Enzo MV, Bedin C, et al. Circulating cell-free DNA: a promising marker of regional lymphonode metastasis in breast cancer patients[J]. Cancer Biomark, 2012, 11(2-3): 89-98. doi: 10.3233/CBM-2012-0263
[12] Tomochika S, Iizuka N, Watanabe Y, et al. Increased serum cell-free DNA levels in relation to inflammation are predictive of distant metastasis of esophageal squamous cell carcinoma[J]. Expe Thera Med, 2010, 1(1): 89-92.
[13] Umetani N, Hiramatsu S, Hoon DSB. Higher Amount of Free Circulating DNA in Serum than in Plasma Is Not Mainly Caused by Contaminated Extraneous DNA during Separation[J]. Annals of the New York Academy of Sciences, 2006, 1075(1075): 299-307.




计量
- 文章访问数: 1352
- HTML全文浏览量: 387
- PDF下载量: 947

