
Evaluation of Postoperative Radiotherapy after Curative Resection in ⅢA-N2 Non-small Cell Lung Cancer with Propensity Score Matching Analysis
-
摘要:目的
分析ⅢA-N2期非小细胞肺癌根治术后辅助放疗(postoperative radiotherapy, PORT)的作用。
方法收集313例非小细胞肺癌根治术后化疗后的ⅢA-N2期患者的临床资料,对PORT(+)组及PORT(-)组资料应用倾向评分匹配方法均衡组间协变量差异,观察两组生存及局控,分析术后放疗的作用及获益人群。
结果匹配后两组患者中,PORT(+)组与PORT(-)组3、5年生存率分别为76.5%、58.3%和52.1%、40.6%(P=0.162);3、5年局部控制率分别为82.9%、73.7%和56.5%、42.4%(P=0.036);3、5年无进展生存率分别为74.8%、65.5%和39.5%、29.6%(P=0.021)。分层分析发现术后放疗可降低隆突下淋巴结转移、肿瘤最大径≥3cm、多站转移、非跳跃转移及术前N2亚组的局部复发风险。
结论术后放疗可提高ⅢA-N2期非小细胞肺癌术后化疗后局部控制率及无进展生存率;亚组分析中隆突下淋巴结转移、肿瘤最大径≥3 cm、多站转移、非跳跃转移及术前N2者获益较大。
Abstract:ObjectiveTo investigate the role of postoperative radiotherapy in the patients treated with curative surgery and adjuvant chemotherapy in stage ⅢA-N2 non-small cell lung cancer (NSCLC).
MethodsThe clinical data of 313 patients pathologically diagnosed as stage ⅢA-N2 NSCLC with curative resection and adjuvant chemotherapy were retrospectively analyzed. Propensity score matching analysis was used to balance the variables differences. The survival and patterns of failure were observed. The role of postoperative radiotherapy and the subgroups that benefited from postoperative radiotherapy were analyzed.
ResultsAfter propensity scores matching, the 3- and 5-year overall survival rates of PORT(+) and PORT(-) were 76.5%, 58.3% and 52.1%, 40.6%, respectively (P=0.162). The 3- and 5-year locoregional control rates of PORT(+) and PORT(-) were 82.9%, 73.7% and 56.5%, 42.4%, respectively (P=0.036). The 3- and 5-year progression-free survival rates of PORT(+) and PORT(-) were 74.8%, 65.5% and 39.5%, 29.6%, respectively (P=0.021). Subgroups analyses suggested that the patients with involvement of subcarinal lymph nodes, tumor diameter≥3cm, multiple N2 metastases, nonskip N2 metastasis and clinical N2 status, and PORT was associated with improved locoregional control rates.
ConclusionPORT could increase the local-regional control rate and progression-free survival rate in stage ⅢA-N2 NSCLC with curative resection and adjuvant chemotherapy; Patients with involvement of subcarinal lymph nodes , tumor diameter≥3cm, multiple N2 metastases, nonskip N2 metastasis and clinical N2 status may benefit most from PORT.
-
0 引言
ⅢA-N2期非小细胞肺癌(non-small cell lung cancer,NSCLC)是备受关注和争议的一组疾病,即使经过完全切除手术及辅助化疗,其局部复发率仍可高达40%[1-4]。随着现代放疗技术的发展,局部放疗的不良反应较前明显减小,但ⅢA-N2期NSCLC完全切除术后辅助放疗的作用仍存在较大争议。本文回顾性分析了ⅢA-N2期NSCLC完全切除术后化疗再放疗与未再放疗患者的生存情况,观察术后放疗的作用及获益人群。
1 资料与方法
1.1 病例资料
自2010年1月至2014年12月于河北医科大学第四医院行手术治疗的ⅢA-N2期NSCLC患者共440例。本研究纳入标准:(1)手术:为可切除NSCLC,行肺癌根治性手术(肺叶切除或全肺切除+纵膈淋巴结清扫术),R0切除,N1及N2站淋巴结清扫站数均≥3站,术后病理为NSCLC,术后病理分期为ⅢA-N2期(按照2009年发布的第七版支气管肺癌TNM分期[5])。(2)化疗:行2周期及以上以铂类为基础的全身辅助化疗。(3)放疗:术后应用6-MV X线行三维适形或调强预防性胸部照射,CTV靶区范围包括手术残端、患侧肺门、受侵淋巴结区域,PTV为CTV外扩0.5 cm,放疗剂量为每日1次,每次2 Gy,5次/周,中位照射剂量为50 Gy(45~54 Gy)。正常组织受量限制:脊髓≤40 Gy,双肺V20≤28%,双肺V30≤18%,心脏V30≤40%,V40≤30%。排除标准:(1)非R0切除;N1或N2淋巴结清扫站数不足3站。(2)行新辅助化疗。(3)术前行胸部放疗。(4)术前已出现远处转移。(5)存在第二原发肿瘤。
1.2 研究方法
入组患者共313例,基本情况见表 1,行术后放疗患者人数较少(仅23例)。为减小选择偏倚,提高研究结果准确性,我们将入组患者采用倾向评分匹配法(propensity score matching,PSM)进行匹配,协变量包括性别、年龄、肿瘤部位、是否术前N2、病理类型、T分期、术式、隆突下淋巴结是否阳性、肿瘤最大径、N2阳性淋巴结个数、N2阳性淋巴结站数以及是否跳跃转移,应用最邻匹配法将术后放疗组和未放疗组患者按1:4进行匹配,对比匹配前后两组间协变量的分布情况。回顾性分析匹配成功患者的病历资料,比较术后放疗组及未放疗组患者生存率、局部控制率、无远转率及无进展率,观察相关临床及病理因素对局控的影响,分析术后放疗作用及获益人群。
表 1 313例ⅢA-N2期非小细胞肺癌患者基本资料Table 1 Clinical characteristics of 313 patients
1.3 观察指标
总生存时间(overall survival,OS)定义为从首治之日开始至患者死亡时间或末次随访日。局部控制时间,即无局部区域复发时间(local-regional failure free survival,LRFFS)定义为从手术之日至患者出现手术残端复发和(或)纵膈淋巴结区域复发的时间。无远处转移时间(distant metastasis free survival,DMFS)定义为从患者手术之日至出现远处转移的时间。无进展生存时间(progression-free survival,PFS)定义为从手术之日开始至第一次发生疾病进展或死亡的时间。根据RTOG放射性损伤分级标准评价术后放疗组患者放射性肺炎、放射性食管炎等不良反应。
1.4 随访与统计学方法
随访时间为手术结束至末次随访或死亡时间。随访方式有门诊复查、再次入院、电话、信访等。随访终止日期为2015年11月5日。统计学分析采用SPSS软件、R2.8.1软件包。应用Kaplan-Meier法计算比较生存率、局部控制率、无远处转移率及无进展生存率,应用Log rank检验分析各变量与预后的关系,应用t检验或χ2检验进行组间分布比较。P<0.05为差异有统计学意义。
2 结果
2.1 匹配前后资料及配比后失败分析
经倾向评分匹配后共103例患者匹配成功,其中术后放疗即PORT(+)组22例,未放疗即PORT(-)组81例,中位随访时间为38.8月,匹配前后基本资料,见表 2。两组患者死亡、局部复发和(或)远处转移例数以及占各组总例数的比例,见表 3。
表 2 倾向评分匹配前后基本资料Table 2 Comparison of characteristics before and after propensity score matching 表 3 配比后103例患者失败情况Table 3 The 103 failure cases after matching
表 3 配比后103例患者失败情况Table 3 The 103 failure cases after matching
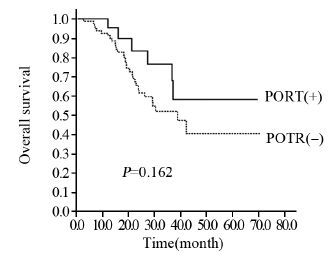
2.2 术后PORT(-)组与PORT(+)组生存比较
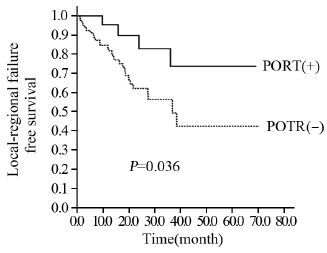
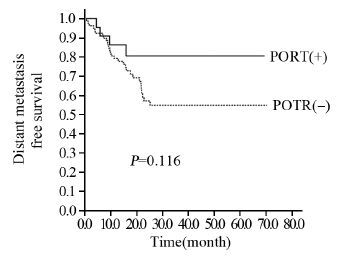
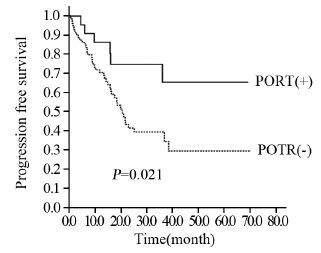
PORT(-)组与PORT(+)组1、3、5年生存率分别为92.5%、52.1%、40.6%与95.5%、76.5%、58.3%(P=0.162),见图 1。PORT(-)组与PORT(+)组1、3、5年局控率分别为83.3%、56.5%、42.4%与95.5%、82.9%、73.7%(P=0.036),见图 2。PORT(-)组与PORT(+)组1、3、5年无远处转移率分别为79.3%、54.9%、54.9%与86.4%、80.6%、80.6%(P=0.116),见图 3。PORT(-)组与PORT(+)组1、3、5年无进展率分别为70.6%、39.5%、29.6%与86.4%、74.8%、65.5%(P=0.021),见图 4。
![]() 图 2 PORT(+)组与PORT(-)组的局控曲线Figure 2 Kaplan-Meier curves for local-regional failure free survival (LRFFS) of PORT(+) and PORT(-)
图 2 PORT(+)组与PORT(-)组的局控曲线Figure 2 Kaplan-Meier curves for local-regional failure free survival (LRFFS) of PORT(+) and PORT(-)![]() 图 3 PORT(+)组与PORT(-)组的无远处转移生存曲线Figure 3 Kaplan-Meier curves for distant metastasis free surival (DMFS) of PORT(+) and PORT(-)
图 3 PORT(+)组与PORT(-)组的无远处转移生存曲线Figure 3 Kaplan-Meier curves for distant metastasis free surival (DMFS) of PORT(+) and PORT(-)![]() 图 4 PORT(+)组与PORT(-)组的无进展生存曲线Figure 4 Kaplan-Meier curves for PFS of PORT(+) and PORT(-)
图 4 PORT(+)组与PORT(-)组的无进展生存曲线Figure 4 Kaplan-Meier curves for PFS of PORT(+) and PORT(-)2.3 术后PORT(-)组与PORT(+)组生存率、局部控制率的分层分析
2.3.1 生存分析
隆突下阳性淋巴结患者PORT(-)组与PORT(+)组3年生存率分别为32.7%、72.9%(P=0.026);隆突下阴性淋巴结患者PORT(-)组与PORT(+)组3年生存率分别为67.0%、68.4%(P=0.565)。术前N2患者PORT(+)组与PORT(+)组3年生存率分别为31.8%、100%(P=0.014);非术前N2患者PORT(-)组与PORT(+)组3年生存率分别为55.0%、45.7%(P=0.448)。对病理类型、阳性N2淋巴结个数与站数、肿瘤最大径及是否跳跃转移的分层分析中,生存率差异均无统计学意义。
2.3.2 局部控制率分析
术后PORT(-)组与PORT(+)组局部控制率的分层分析,见表 4。亚组分析中,隆突下淋巴结阳性、多站N2阳性淋巴结、肿瘤最大径>3 cm及非跳跃转移患者的局部控制率PORT(+)组高于与 PORT(-)组,P值分别为0.011、0.038、0.046和0.034。
表 4 PORT(+)组与PORT(-)组局控的分层分析Table 4 Hierarchical analysis for LRFFS of PORT(+) and PORT(-)
2.4 放疗不良反应
随访期内,术后放疗组共22例ⅢA-N2期NSCLC患者中,仅有1例发生2级放射性肺炎(4.5%),2例发生Ⅱ度及以下骨髓抑制(9.1%),未发现放射性食管炎及放射性心包炎,未发现3级或4级放射性损伤。
3 讨论
近年来许多文献报道了术后放疗可提高ⅢA-N2期NSCLC患者总生存。Zou等通过多中心回顾性分析了ⅢA-N2期NSCLC完全切除术后放疗的作用,结果显示术后放疗提高了ⅢA-N2期NSCLC患者5年生存率(P=0.007)[6]。Robinson等研究报道了pN2期NSCLC完全切除术后放化疗组与术后单纯化疗组5年生存率分别为39.3%与34.8%(P=0.014)[7]。Lally等发现术后放疗可使pN2期NSCLC术后5年生存率提高7%(P=0.008)[8]。Feng等报道了ⅢA-N2期NSCLC术后预防性胸部照射可得到明显的生存获益[9]。
Dai等报道了ⅢA-N2期NSCLC完全切除后辅助放疗组与未辅助放疗组的5年局部控制率分别为63.9%、46.7%(P=0.025)[10]。刘翼等报道术后辅助放疗可降低ⅢA-N2期NSCLC术后化疗后局部复发风险(P=0.001)[11]。Kim等应用PSM评价ⅢA-N2期NSCLC术后放疗的作用,结果发现术后放疗显著提高了ⅢA-N2期NSCLC的局部控制率,而未延长总生存期[12],本研究中术后放疗组局部控制率优于未放疗组,与上述文献结果相近。
目前,一些学者研究术后放疗在ⅢA-N2期NSCLC各因素亚组中的作用,观察获益人群。其中,Matsuguma等报道应用现代放疗技术可提高多站转移的ⅢA-N2期NSCLC的5年无病生存率,降低局部复发风险[13]。Sawyer等认为N2多站转移是ⅢA-N2期NSCLC术后复发的高级风险因素,T3、T4是ⅢA-N2期NSCLC术后复发的中级风险因素,均可获益于术后胸部放疗[14]。杜芳芳等研究发现多站转移的pN2期NSCLC患者中放疗组与未放疗组5年生存率和5年局部控制率分别为36%、20%(P=0.013)和65%、48%(P=0.006);肿瘤最大直径>3cm的患者中放疗组与未放疗组5年生存率和5年局部控制率分别为33%、15%(P=0.002)和62%、48%(P=0.033)[15]。Saito等报道了肿瘤直径>2 cm的pN2期NSCLC的5年生存率远低于≤2cm的患者[16]。本研究结果亦发现多站转移、肿瘤最大直径≥3cm亚组可获益于术后放疗,使复发风险降低。
对于隆突下淋巴结阳性的亚组,Aokage等发现对比隆突下淋巴结阴性的NSCLC,隆突下淋巴结阳性者更易出现复发,且5年生存率较低[17]。刘敬伟等研究报道存在隆突下淋巴结转移的ⅢA-N2期NSCLC术后复发风险是未转移者的2.11倍(P=0.026)[18]。在本研究中,隆突下淋巴结阳性的ⅢA-N2期NSCLC行术后化疗再辅以放疗可提高生存率,降低复发风险。鉴于隆突下淋巴结转移者可能导致复发高预后差的特点,我们建议术后放疗应引起足够重视。目前许多研究报道pN2期NSCLC中淋巴结跳跃转移者预后优于无跳跃转移者,生存率较高,但具体机制尚不明确[19-22]。有学者认为跳跃转移组的淋巴结转移总个数往往低于非跳跃组,在淋巴引流中肿瘤负荷较小,因此可致较好的生存和较低的复发[23]。此外,Kim等报道术后放疗提高了ⅢA-N2期NSCLC中鳞癌亚组的5年局部控制率[12],靳国华等也有相似的报道[24]。在本研究结果中,鳞癌亚组术后放疗者3、5年局部控制率均高于未术后放疗者,差异接近统计学意义(P=0.055)。
综上分析,术后放疗可提高ⅢA-N2期NSCLC术后化疗后局部控制率及无进展生存率;亚组分析中隆突下淋巴结转移、肿瘤最大径≥3 cm、多站转移、非跳跃转移及术前N2者获益较大。我们建议ⅢA-N2期NSCLC术后化疗后行预防性胸部放疗,尤其是受益较大的亚组。但本文是回顾性研究,术后放疗人数仅22例,尤其是分层分析中各层例数均较少,代表性可能较差,虽然整体匹配后两组差异明显减小,基线水平基本一致,但匹配后标准化均数差(SMD)还有三项大于0.1,匹配并非较高水平。因此,ⅢA-N2期NSCLC术后放疗的作用及获益人群仍需大样本前瞻性研究做进一步分析及验证。
-
![]()
图 2 PORT(+)组与PORT(-)组的局控曲线
Figure 2 Kaplan-Meier curves for local-regional failure free survival (LRFFS) of PORT(+) and PORT(-)
![]()
图 3 PORT(+)组与PORT(-)组的无远处转移生存曲线
Figure 3 Kaplan-Meier curves for distant metastasis free surival (DMFS) of PORT(+) and PORT(-)
![]()
图 4 PORT(+)组与PORT(-)组的无进展生存曲线
Figure 4 Kaplan-Meier curves for PFS of PORT(+) and PORT(-)
表 2 倾向评分匹配前后基本资料
Table 2 Comparison of characteristics before and after propensity score matching
 下载: 导出CSV
下载: 导出CSV
表 4 PORT(+)组与PORT(-)组局控的分层分析
Table 4 Hierarchical analysis for LRFFS of PORT(+) and PORT(-)
下载: 导出CSV
-
[1] NSCLC Meta-analyses Collaborative Group, Arriagada R, Auprrin A, et al. Ajuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer:Two meta-analyses of individual patient data[J]. Lancet, 2010, 375: 1267-77. doi: 10.1016/S0140-6736(10)60059-1
[2] Le Péchoux C. Role of postoperative radiotherapy in resected non-small cell lung cancer: a reassessment based on new data[J]. Oncologist, 2011, 16(5): 672-81. doi: 10.1634/theoncologist.2010-0150
[3] Douillard JY, Rosell R, De Lena M, et al. Impact of postoperative radiation therapy on survival in patients with complete resection and stage Ⅰ, Ⅱ, or ⅢA non-small-cell lung cancer treated with adjuvant chemotherapy: the adjuvant Navelbine International Trialist Association (ANITA) Randomized Trial[J]. Int J Radiat Oncol Biol Phys, 2008, 72(3): 695-701. doi: 10.1016/j.ijrobp.2008.01.044
[4] Arriagada R, Bergman B, Dunant A, et al. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer[J]. N Engl J Med, 2004, 350(4): 351-60. doi: 10.1056/NEJMoa031644
[5] Detterbeck FC, Boffa DJ, Tanoue LT. The New Lung Cancer Staging System[J]. Chest, 2009, 136(1): 260-71. doi: 10.1378/chest.08-0978
[6] Zou B, Xu Y, Li T, et al. A multicenter retrospective analysis of survival outcome following postoperative chemoradiotherapy in non-small-cell lung cancer patients with N2 nodal disease[J]. Int J Radiat Oncol Biol Phys, 2010, 77(2): 321-8. doi: 10.1016/j.ijrobp.2009.05.044
[7] Robinson CG, Patel AP, Bradley JD, et al. Postoperative radiotherapy for pathologic N2 non-small-cell lung cancer treated with adjuvant chemotherapy: a review of the National Cancer Data Base[J]. J Clin Oncol, 2015, 33(8): 870-6. doi: 10.1200/JCO.2014.58.5380
[8] Lally BE, Zelterman D, Colasanto JM, et al. Postoperative radiotherapy for stage Ⅱ or Ⅲ non-small-cell lung cancer using the surveillance, epidemiology, and end results database[J]. J Clin Oncol, 2006, 24(19): 2998-3006. doi: 10.1200/JCO.2005.04.6110
[9] Feng W, Zhang Q, Fu XL, et al. The emerging outcome of postoperative radiotherapy for stage ⅢA(N2) non-small cell lung cancer patients: based on the three-dimensional conformal radiotherapy technique and institutional standard clinical target volume[J]. BMC Cancer, 2015, 15(1): 1-10. doi: 10.1186/1471-2407-15-1
[10] Dai HH, Hui ZG, Ji W, et al. Postoperative radiotherapy for resected pathological stage ⅢA-N2 non-small cell lung cancer:a retrospective study of 211 cases from a single institution[J]. Lung Cancer, 2011, 16(5): 641-50.
[11] 刘翼, 阿迪力, 陆艳荣, 等. ⅢA(N2)期非小细胞肺癌术后放疗疗效分析[J].中国癌症杂志, 2013, 23(6): 452-6. http://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ201306011.htm Liu Y, A DL, Lu YR, et al. Analyze the curative effect of adjuwant radiotherapy in stage ⅢA(N2) non-small cell lung cancer[J]. Zhongguo Ai Zheng Za Zhi, 2013, 23(6): 452-6. http://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ201306011.htm
[12] Kim BH, Kim HJ, Wu HG, et al. Role of postoperative radiotherapy after curative resection and adjuvant chemotherapy for patients with pathological stage N2 non-small-cell lung cancer: a propensity score matching analysis[J]. Clin Lung Cancer, 2014, 15(5): 356-64. doi: 10.1016/j.cllc.2014.05.005
[13] Matsuguma H, Nakahara R, Ishikawa Y, et al. Postoperative radiotherapy for patients with completely resected pathological stage ⅢA-N2 non-small cell lung cancer: focusing on an effect of the number of mediastinal lymph node stations involved[J]. Interact Cardiovasc Thorac Surg, 2008, 7(4): 573-7. doi: 10.1510/icvts.2007.174342
[14] Sawyer TE, Bonner JA, Gould PM, et al. Effectiveness of postoperative irradiation in stage ⅢA non-small cell lung cancer according to regression tree analyses of recurrence risks[J]. Ann Thorac Surg, 1997, 64(5): 1402-7. doi: 10.1016/S0003-4975(97)00908-9
[15] 杜芳芳, 袁智勇, 王军, 等. 术后放射治疗在pN2期非小细胞肺癌中的地位[J]. 中国肺癌杂志, 2009, 12(11): 1164-8. http://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ200911009.htm Du FF, Yuan ZY, Wang J, et al. The Role of Postoperative Radiotherapy on Stage N2 Non-small Cell Lung Cancer[J]. Zhongguo Fei Ai Za Zhi, 2009, 12(11): 1164-8. http://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ200911009.htm
[16] Saito M, Kato H. Prognostic factors in patients with pathological and N2 non-small cell lung cancer[J]. Ann Thorac Cardiovasc Surg, 2008, 14(1): 1-2.
[17] Aokage K, Yoshida J, Ishii G, et al. Subcarinal lymph node in upper lobe non-small cell lung cancer patients: is selective lymph node dissection valid?[J]. Lung Cancer, 2010, 70(2): 163-7. doi: 10.1016/j.lungcan.2010.02.009
[18] 刘敬伟, 李简, 林钢, 等. ⅢA-N2期非小细胞肺癌根治性切除术后的复发分析[J]. 中华医学杂志, 2012, 92(33): 2314-8. Liu JW, Li J, Lin G, et al. Analysis of recurrence patterns after curative resection of stage ⅢA-N2 non-small cell lung cancer[J]. Zhonghua Yi Xue Za Zhi, 2012, 92(33): 2314-8.
[19] Nakagiri T, Sawabata N, Funaki S, et al. Validation of pN2 sub-classifications in patients with pathological stage ⅢA N2 non-small cell lung cancer[J]. Interact Cardiovasc Thorac Surg, 2011, 12(5): 733-8. doi: 10.1510/icvts.2010.249896
[20] 张连民, 张真发, 王长利, 等.ⅢA-N2期非小细胞肺癌纵膈淋巴结跳跃式转移的临床和预后分析[J]. 中华外科杂志, 2010, 48(10): 780-3. Zhang LM, Zhang ZF, Wang CL, et al. Clinical and prognostic analysis of skip N2 metastases in stage ⅢA-N2 non-small cell lung cancer[J]. Zhonghua Wai Ke Za Zhi, 2010, 48(10): 780-3.
[21] Sonobe M, Date H, Wada H, et al. Prognostic factors after complete resection of pN2 non-small cell lung cancer[J]. J Thorac Cardiovasc Surg, 2013, 146(4): 788-95. doi: 10.1016/j.jtcvs.2013.04.043
[22] 曹勤琛, 张宝忠, 王长利, 等. ⅢA-N2期非小细胞肺癌纵膈淋巴结转移综合模式的预后价值[J]. 中国肿瘤临床, 2014, 41(20): 1312-6. http://www.cnki.com.cn/Article/CJFDTOTAL-ZGZL201420016.htm Cao QC, Zhang BZ, Wang CL, et al. The prognostic value of a combined pattern of mediastinal lymph node metastasis for ⅢA-N2 non-small-cell lung cancer[J]. Zhongguo Zhong Liu Lin Chuang, 2014, 41(20): 1312-6. http://www.cnki.com.cn/Article/CJFDTOTAL-ZGZL201420016.htm
[23] Wei S, Asamura H, Kawachi R, et al. Which is the better prognostic factor for resected non-small cell lung cancer the number of metastatic lymph nodes or the currently used nodal stage classification?[J]. J Thorac Oncol, 2011, 6(2): 310-8. doi: 10.1097/JTO.0b013e3181ff9b45
[24] 靳国华, 刘桂梅, 夏广蓉, 等. ⅢA期非小细胞肺癌术后辅助放射治疗疗效分析[J]. 中华放射肿瘤学杂志, 2001, 10(2): 97-9. Jin GH, Liu GM, Xia GR, et al. Postoperative radiotherapy for stage ⅢA non-small cell lung carcinoma[J]. Zhonghua Fang She Zhong Liu Xue Za Zhi, 2001, 10(2): 97-9.
计量
- 文章访问数: 1199
- HTML全文浏览量: 361
- PDF下载量: 407

